My first day at the hospital today, and it is very different to the UK (though no surprises there). The highlight today was unpacking the medication boxes I had bought with me from the UK. The quantity of medicines was huge, and a number of drugs we had tried to prescribe during the morning ward round, only to be told they had run out (such as amoxicillin) were present in their thousands. A very happy pharmacist and head of hospital. I feel as though I am helping already and I haven't done anything!.

Enough drugs came in those two boxes to keep a crack house running for a year...
But wait, when I was saying "we tried to prescribe", l wasn't using 'we' the normal way I do in this blog, where I mean the doctor and med students discuss which drug should be used, then the doctor tells the students that they are (most likely) wrong then prescribes the correct drug. Here the ward round was conducted by us three medical students with an 18 year old student nurse to act as a translator. This is petrifying. Doctors only do ward rounds Monday, Wednesday and Friday, so the other days the ward is just left to run with nurses giving out medication. If it is prescribed. This means we students currently do the ward rounds on the other days of the week, or they are not done. Supposedly doctors can often miss a weekday ward round as well, if something comes up, so foreign medical students are very useful to keep seeing the patients...
The working day Starts at 7.30 with prayers for half an hour, though today I went straight for the meeting which starts at 8 to discuss new admissions and changes to patients conditions. While in Swahili, all Medical words are in English, so I can still understand the gist of what is happening. I Just hear "Blah Blah Blah 'hypertension Blah Blah normal saline"... After this the doctors and nurses take breakfast, then ward rounds are meant to Start at 9. This seems very important as the lab and the pharmacy close at 2, meaning that no tests or medicine can be given after 2PM unless there is an emergency, where the pharmacist / lab tec is called from home to come in and help.
The medical students explain to me that this means that if a patient is admitted on Friday after the ward round, they may not see a doctor until Monday, perhaps around 11 if he is running late (not uncommon), which means that by the time the investigation requests are sent to the lab, there may be not enough time to process them before the lab Closes at 2, so it is only by Wednesday, 5 days after the admission that the patient may receive the necessary medication. This is a 'worst case Scenario' and if the patient seems acutely ill (has to be noticed by the nursing students) they can call a doctor to come in and see the patient at any time. Because of the delay there may be in lab tests, results are seldom waited for, (and when they are, not always trusted) and most treatment is empirical, meaning based on guessing the diagnosis. For example, I am told that whether the test for malaria (blood smear looked at under the microscope) is positive or negative, the patient is always given a drug against malaria (I.e. Alu) just in case. This makes doing the blood smear seem a little pointless to me, and I will look into it further...
The working day Starts at 7.30 with prayers for half an hour, though today I went straight for the meeting which starts at 8 to discuss new admissions and changes to patients conditions. While in Swahili, all Medical words are in English, so I can still understand the gist of what is happening. I Just hear "Blah Blah Blah 'hypertension Blah Blah normal saline"... After this the doctors and nurses take breakfast, then ward rounds are meant to Start at 9. This seems very important as the lab and the pharmacy close at 2, meaning that no tests or medicine can be given after 2PM unless there is an emergency, where the pharmacist / lab tec is called from home to come in and help.
The medical students explain to me that this means that if a patient is admitted on Friday after the ward round, they may not see a doctor until Monday, perhaps around 11 if he is running late (not uncommon), which means that by the time the investigation requests are sent to the lab, there may be not enough time to process them before the lab Closes at 2, so it is only by Wednesday, 5 days after the admission that the patient may receive the necessary medication. This is a 'worst case Scenario' and if the patient seems acutely ill (has to be noticed by the nursing students) they can call a doctor to come in and see the patient at any time. Because of the delay there may be in lab tests, results are seldom waited for, (and when they are, not always trusted) and most treatment is empirical, meaning based on guessing the diagnosis. For example, I am told that whether the test for malaria (blood smear looked at under the microscope) is positive or negative, the patient is always given a drug against malaria (I.e. Alu) just in case. This makes doing the blood smear seem a little pointless to me, and I will look into it further...
Today we did ward rounds around the male, the female and the children's wards. Many of the children were in for Malaria or pneumonia (hence the need for amoxicillin) and the adults for a range of illnesses, though also a good few cases of malaria and pneumonia. There were only about 40 people in these three wards, though maternity which we didn't go around had about 80 people in. Three medical students trying to diagnose illnesses and work out which of the limited supply of drugs was appropriate with a BNF and an Oxford Handbook was really not ideal, but fortunately the other two had some experience at this hospital and had a good idea what tests could be done, what drugs were available and what diseases were common. I, however, had a black doll from the IHPUK drugs pack to play with the kids and distract them. Pretty much the only thing I can offer to our team right now...
was really not ideal, but fortunately the other two had some experience at this hospital and had a good idea what tests could be done, what drugs were available and what diseases were common. I, however, had a black doll from the IHPUK drugs pack to play with the kids and distract them. Pretty much the only thing I can offer to our team right now...


My secret weapon, an awesome doll that came with the drugs packs. Perhaps this is because the best medicine is actually laughter...
Two patients I saw today really stuck in my mind. The first was a lady who had been admitted three days ago with two broken wrists from a fall. She had travelled a very long way to get an x-ray (not available at this hospital, and the nearest big hospitals machine was broken) to confirm this, then returned to have them put in casts. Unfortunately there were only the materials for one of the wrists to be put in a plaster of Paris cast. She cannot go home without a cast, and the untreated wrist has just been left for days to sit there out of position. Needless to say this is not good for her, but she is stuck in hospital until a relative makes their way to the nearest town and buys the materials to plaster her other wrist. Such a waste of her time and a hospital bed. I don't know why they didn't make up a temporary cast while waiting, as now she will have to have some kind of procedure before the new cast is fitted, as her bones will have fused while broken, and so will need to be pulled apart and put into the correct position before the cast is fitted. Whenever that may be.
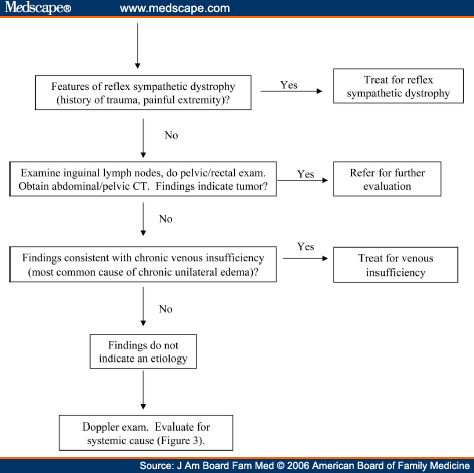
The second patient was a man (Ludwig) who was admitted with right knee pain. Initial diagnosis was osteoarthritis, so we got him to roll up his trousers so we could look at the legs. In addition to flaky peely skin on both legs (very common here, from vitamin deficiency), the right leg had a red and swollen knee, but was also very oedematous (full of fluid and puffy) whereas the left hand leg was practically normal, though it did look very thin and malnourished. Confused as to the potential causes for a young man to have unilateral pitting oedema, we ordered the standard tests (malaria, haemoglobin) and went to look it up. Coming up with a variety of causes we couldn't test for (something I will need to get used to), we went back to perform a full examination. The malaria test was positive, so we started treatment for that (Alu), but didn't really explain the symptoms. History taking from Ludwig is difficult, as he has a relative who is needed to convey what we want to say in Swahili (from the nurse) to the patient, in what I assume is a tribal language. This 3 way translation doesn't seem to bee too accurate, and we get some very unrelated answers back to questions. The examination (that probably should have been done by the doctor who admitted him) showed abdominal ascites (fluid in the belly) with very thin arms to match his thin leg. Very strange. With the thin arms and leg we decided it would be worth using a bedside HlV test on him (HIV is also known as slim disease) to check whether he has HIV. The prevalence here is around 6%, so adults are not checked routinely, but unfortunately this turned out to be a good guess, as he was HIV positive. Unsure who should tell him we left the nurses to sort it out in a cowardly move, though in our defence, we were unsure how we could help, given our lack of language. Terrible to diagnose someone with this disease, and even more terrible to run away before telling them... But still a diagnosis from our medical student team, which hopefully means he can now be treated properly. Good work!


The very nice house we stayed in. with a solar panel on the roof and wires connecting it to the hospital's batteries. We came back here after each day for dinner, and sleep.
Tomorrow I have planned to go on a medical Safari which should be very exciting. Lots of vaccinations, weighing children and checking on pregnant mothers (Anti-natal checks).


{kind=link}
No comments:
Post a Comment